Do Fallen Arches Need Surgery?
Overview

A variety of foot problems can lead to adult acquired flatfoot deformity (AAFD), a condition that results in a fallen arch with the foot pointed outward. Most people - no matter what the cause of their flatfoot - can be helped with orthotics and braces. In patients who have tried orthotics and braces without any relief, surgery can be a very effective way to help with the pain and deformity. This article provides a brief overview of the problems that can result in AAFD. Further details regarding the most common conditions that cause an acquired flatfoot and their treatment options are provided in separate articles. Links to those articles are provided.
Causes
Genetic predisposition. Faulty foot mechanics, e.g. excessive pronation. Abnormal bony architecture. Laxity of ligaments. Neuro-muscular disease. Trauma to the leg muscles or major tendons. Inflammatory diseases of the joints e.g. Rheumatoid arthritis. Surgical procedures on the leg and ankle. Limb length inequality. Tight Achilles tendon.
Symptoms
Flat feet can cause a myriad of symptoms, from experiencing pain in the foot, heels, arch, calves, the shin, the knee, the hip and into the lower back due to overworking of the hip flexors or they may find it hard to stand on tip toes.
Diagnosis
There are a few simple ways to assess your foot type, and most include making an imprint of your footprint. The classic way is to stand on a hard floor surface with wet feet to make a wet foot print. Look at the narrowest part of your footprint, which should be between your heel and ball of your foot. If the print of your foot in this part is less than 10% of the width of the widest part then you are likely to have high arches. more than 10% but less than 25% then your foot profile is probably normal, more than 25% or even the widest part, then you have flat feet.
Is flat footedness genetic?
Non Surgical Treatment
Flexible flat feet that are painless do not require treatment. If you have pain due to flexible flat feet, an orthotic (arch-supporting insert in the shoe) can bring relief. With the increased interest in running, many shoe stores carry shoes for normal feet and pronated feet. The shoes designed for pronated feet make long distance running easier and less tiring because they correct for the abnormality. Rigid or painful flat feet require evaluation by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. If this fails to improve the pain, surgery may be necessary. For problems with the posterior tibial tendon, treatment may start with rest, anti-inflammatory medications, and shoe inserts or ankle braces. In more advanced cases, surgery may be needed to clean or repair the tendon, or fuse some of the joints of the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment

Surgery is typically offered as a last resort in people with significant pain that is resistant to other therapies. The treatment of a rigid flatfoot depends on its cause. Congenital vertical talus. Your doctor may suggest a trial of serial casting. The foot is placed in a cast and the cast is changed frequently to reposition the foot gradually. However, this generally has a low success rate. Most people ultimately need surgery to correct the problem. Tarsal coalition. Treatment depends on your age, extent of bone fusion and severity of symptoms. For milder cases, your doctor may recommend nonsurgical treatment with shoe inserts, wrapping of the foot with supportive straps or temporarily immobilizing the foot in a cast. For more severe cases, surgery is necessary to relieve pain and improve the flexibility of the foot. Lateral subtalar dislocation. The goal is to move the dislocated bone back into place as soon as possible. If there is no open wound, the doctor may push the bone back into proper alignment without making an incision. Anesthesia is usually given before this treatment. Once this is accomplished, a short leg cast must be worn for about four weeks to help stabilize the joint permanently. About 15% to 20% of people with lateral subtalar dislocation must be treated with surgery to reposition the dislocated bone.
Prevention
Going barefoot, particularly over terrain such as a beach where muscles are given a good workout, is good for all but the most extremely flatfooted, or those with certain related conditions such as plantar fasciitis. Ligament laxity is also among the factors known to be associated with flat feet. One medical study in India with a large sample size of children who had grown up wearing shoes and others going barefoot found that the longitudinal arches of the bare footers were generally strongest and highest as a group, and that flat feet were less common in children who had grown up wearing sandals or slippers than among those who had worn closed-toe shoes. Focusing on the influence of footwear on the prevalence of pes planus, the cross-sectional study performed on children noted that wearing shoes throughout early childhood can be detrimental to the development of a normal or a high medial longitudinal arch. The vulnerability for flat foot among shoe-wearing children increases if the child has an associated ligament laxity condition. The results of the study suggest that children be encouraged to play barefooted on various surfaces of terrain and that slippers and sandals are less harmful compared to closed-toe shoes. It appeared that closed-toe shoes greatly inhibited the development of the arch of the foot more so than slippers or sandals. This conclusion may be a result of the notion that intrinsic muscle activity of the arch is required to prevent slippers and sandals from falling off the child?s foot.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
A variety of foot problems can lead to adult acquired flatfoot deformity (AAFD), a condition that results in a fallen arch with the foot pointed outward. Most people - no matter what the cause of their flatfoot - can be helped with orthotics and braces. In patients who have tried orthotics and braces without any relief, surgery can be a very effective way to help with the pain and deformity. This article provides a brief overview of the problems that can result in AAFD. Further details regarding the most common conditions that cause an acquired flatfoot and their treatment options are provided in separate articles. Links to those articles are provided.
Causes
Genetic predisposition. Faulty foot mechanics, e.g. excessive pronation. Abnormal bony architecture. Laxity of ligaments. Neuro-muscular disease. Trauma to the leg muscles or major tendons. Inflammatory diseases of the joints e.g. Rheumatoid arthritis. Surgical procedures on the leg and ankle. Limb length inequality. Tight Achilles tendon.
Symptoms
Flat feet can cause a myriad of symptoms, from experiencing pain in the foot, heels, arch, calves, the shin, the knee, the hip and into the lower back due to overworking of the hip flexors or they may find it hard to stand on tip toes.
Diagnosis
There are a few simple ways to assess your foot type, and most include making an imprint of your footprint. The classic way is to stand on a hard floor surface with wet feet to make a wet foot print. Look at the narrowest part of your footprint, which should be between your heel and ball of your foot. If the print of your foot in this part is less than 10% of the width of the widest part then you are likely to have high arches. more than 10% but less than 25% then your foot profile is probably normal, more than 25% or even the widest part, then you have flat feet.
Is flat footedness genetic?
Non Surgical Treatment
Flexible flat feet that are painless do not require treatment. If you have pain due to flexible flat feet, an orthotic (arch-supporting insert in the shoe) can bring relief. With the increased interest in running, many shoe stores carry shoes for normal feet and pronated feet. The shoes designed for pronated feet make long distance running easier and less tiring because they correct for the abnormality. Rigid or painful flat feet require evaluation by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. If this fails to improve the pain, surgery may be necessary. For problems with the posterior tibial tendon, treatment may start with rest, anti-inflammatory medications, and shoe inserts or ankle braces. In more advanced cases, surgery may be needed to clean or repair the tendon, or fuse some of the joints of the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery.
Surgical Treatment
Surgery is typically offered as a last resort in people with significant pain that is resistant to other therapies. The treatment of a rigid flatfoot depends on its cause. Congenital vertical talus. Your doctor may suggest a trial of serial casting. The foot is placed in a cast and the cast is changed frequently to reposition the foot gradually. However, this generally has a low success rate. Most people ultimately need surgery to correct the problem. Tarsal coalition. Treatment depends on your age, extent of bone fusion and severity of symptoms. For milder cases, your doctor may recommend nonsurgical treatment with shoe inserts, wrapping of the foot with supportive straps or temporarily immobilizing the foot in a cast. For more severe cases, surgery is necessary to relieve pain and improve the flexibility of the foot. Lateral subtalar dislocation. The goal is to move the dislocated bone back into place as soon as possible. If there is no open wound, the doctor may push the bone back into proper alignment without making an incision. Anesthesia is usually given before this treatment. Once this is accomplished, a short leg cast must be worn for about four weeks to help stabilize the joint permanently. About 15% to 20% of people with lateral subtalar dislocation must be treated with surgery to reposition the dislocated bone.
Prevention
Going barefoot, particularly over terrain such as a beach where muscles are given a good workout, is good for all but the most extremely flatfooted, or those with certain related conditions such as plantar fasciitis. Ligament laxity is also among the factors known to be associated with flat feet. One medical study in India with a large sample size of children who had grown up wearing shoes and others going barefoot found that the longitudinal arches of the bare footers were generally strongest and highest as a group, and that flat feet were less common in children who had grown up wearing sandals or slippers than among those who had worn closed-toe shoes. Focusing on the influence of footwear on the prevalence of pes planus, the cross-sectional study performed on children noted that wearing shoes throughout early childhood can be detrimental to the development of a normal or a high medial longitudinal arch. The vulnerability for flat foot among shoe-wearing children increases if the child has an associated ligament laxity condition. The results of the study suggest that children be encouraged to play barefooted on various surfaces of terrain and that slippers and sandals are less harmful compared to closed-toe shoes. It appeared that closed-toe shoes greatly inhibited the development of the arch of the foot more so than slippers or sandals. This conclusion may be a result of the notion that intrinsic muscle activity of the arch is required to prevent slippers and sandals from falling off the child?s foot.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Heel Serious Pain The Causes, Warning Signs And Cure Options
Overview
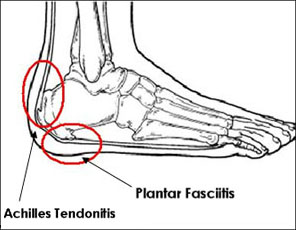
As anyone who has ever had foot pain can tell you, when your feet hurt, you hurt all over. ?The feet are the foundation of our ?building,? or body,? says Craig Gastwirth, a podiatrist at Podiatry Examiners of Michigan in Detroit. ?If there?s a problem with that foundation, everything else - knees, hips and back - is thrown off.? Heel pain, typically caused by plantar fasciitis, is the No. 1 reason people visit a podiatrist, says Dr. Gastwirth. Plantar fasciitis, inflammation of a thick band of connective tissue called the plantar fascia, which runs along the sole from the bottom of the heel bone to the toes, can feel like the arch of the foot is tearing.
Causes
Plantar fasciitis: It is the most common cause of heel pain. In this condition, the pain is more severe in the morning but becomes less painful as the day continues. It occurs due to tiny tears in the plantar fascia.The plantar faschia is a tissue band that connects the bottom of the heel bones to the ball of the foot and is involved in walking and running, giving spring to the step. If left untreated, the symptoms usually worsen and can lead to problems with the knee and hip and can cause back pain due to difficulty walking. Those who frequently stand or walk throughout the day or those who run are most likely to develop plantar fasciitis.
Symptoms
The primary symptom is pain in the heel area that varies in severity and location. The pain is commonly intense when getting out of bed or a chair. The pain often lessens when walking.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
Initial treatment should consist of an ice pack. Some runners prefer to use a wet towel that has been in the fridge. We recommend you use commercially available ice packs for focused pain released. An anti-inflammatory such as Ibuprofen will help to reduce the swelling. Please note this should be taken with meals and never before running. As with all soft tissue injuries, you may have to re-examine your training regime. A reduction or even a total break form running may be necessary. . Examine your running shoes, making sure the shoes do not bend excessively near the middle of the foot and at the ball of the foot. Sports shoes with built in insoles can be beneficial, however we recommend you replace existing insoles with specific sports orthotics/ insoles. Silicone heel cups, leather heel pads and contrasting cold and hot therapy can all help to speed up the healing process. The plantar fascia stretch will help to prevent the injury from occurring again. Please note that this stretch should not be done while the heel is inflamed and should only be attempted once you?re a feeling minimal or no pain from your heel.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
heel pain cure
Prevention

Wear shoes that fit well, front, back and sides and have shock-absorbent soles, rigid uppers and supportive heel counters. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm-up before running or walking, and do some stretching exercises afterward. Pace yourself when you participate in athletic activities. If overweight, try non weight-bearing activities such as swimming or cycling. Your podiatrist may also use taping or strapping to provide extra support for your foot. Orthoses (shoe inserts) specifically made to suit your needs may be also be prescribed.
As anyone who has ever had foot pain can tell you, when your feet hurt, you hurt all over. ?The feet are the foundation of our ?building,? or body,? says Craig Gastwirth, a podiatrist at Podiatry Examiners of Michigan in Detroit. ?If there?s a problem with that foundation, everything else - knees, hips and back - is thrown off.? Heel pain, typically caused by plantar fasciitis, is the No. 1 reason people visit a podiatrist, says Dr. Gastwirth. Plantar fasciitis, inflammation of a thick band of connective tissue called the plantar fascia, which runs along the sole from the bottom of the heel bone to the toes, can feel like the arch of the foot is tearing.
Causes
Plantar fasciitis: It is the most common cause of heel pain. In this condition, the pain is more severe in the morning but becomes less painful as the day continues. It occurs due to tiny tears in the plantar fascia.The plantar faschia is a tissue band that connects the bottom of the heel bones to the ball of the foot and is involved in walking and running, giving spring to the step. If left untreated, the symptoms usually worsen and can lead to problems with the knee and hip and can cause back pain due to difficulty walking. Those who frequently stand or walk throughout the day or those who run are most likely to develop plantar fasciitis.
Symptoms
The primary symptom is pain in the heel area that varies in severity and location. The pain is commonly intense when getting out of bed or a chair. The pain often lessens when walking.
Diagnosis
Your doctor will perform a physical exam and ask questions about your medical history and symptoms, such as have you had this type of heel pain before? When did your pain begin? Do you have pain upon your first steps in the morning or after your first steps after rest? Is the pain dull and aching or sharp and stabbing? Is it worse after exercise? Is it worse when standing? Did you fall or twist your ankle recently? Are you a runner? If so, how far and how often do you run? Do you walk or stand for long periods of time? What kind of shoes do you wear? Do you have any other symptoms? Your doctor may order a foot x-ray. You may need to see a physical therapist to learn exercises to stretch and strengthen your foot. Your doctor may recommend a night splint to help stretch your foot. Surgery may be recommended in some cases.
Non Surgical Treatment
Initial treatment should consist of an ice pack. Some runners prefer to use a wet towel that has been in the fridge. We recommend you use commercially available ice packs for focused pain released. An anti-inflammatory such as Ibuprofen will help to reduce the swelling. Please note this should be taken with meals and never before running. As with all soft tissue injuries, you may have to re-examine your training regime. A reduction or even a total break form running may be necessary. . Examine your running shoes, making sure the shoes do not bend excessively near the middle of the foot and at the ball of the foot. Sports shoes with built in insoles can be beneficial, however we recommend you replace existing insoles with specific sports orthotics/ insoles. Silicone heel cups, leather heel pads and contrasting cold and hot therapy can all help to speed up the healing process. The plantar fascia stretch will help to prevent the injury from occurring again. Please note that this stretch should not be done while the heel is inflamed and should only be attempted once you?re a feeling minimal or no pain from your heel.
Surgical Treatment
With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick.
heel pain cure
Prevention
Wear shoes that fit well, front, back and sides and have shock-absorbent soles, rigid uppers and supportive heel counters. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm-up before running or walking, and do some stretching exercises afterward. Pace yourself when you participate in athletic activities. If overweight, try non weight-bearing activities such as swimming or cycling. Your podiatrist may also use taping or strapping to provide extra support for your foot. Orthoses (shoe inserts) specifically made to suit your needs may be also be prescribed.
Leg Length Discrepancy Surgery Cost
Overview
Surgical options in leg length discrepancy treatment include procedures to lengthen the shorter leg, or shorten the longer leg. Your child's physician will choose the safest and most effective method based on the aforementioned factors. No matter the surgical procedure performed, physical therapy will be required after surgery in order to stretch muscles and help support the flexibility of the surrounding joints. Surgical shortening is safer than surgical lengthening and has fewer complications. Surgical procedures to shorten one leg include removing part of a bone, called a bone resection. They can also include epiphysiodesis or epiphyseal stapling, where the growth plate in a bone is tethered or stapled. This slows the rate of growth in the surgical leg.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
The patient/athlete may present with an altered gait (such as limping) and/or scoliosis and/or low back pain. Lower extremity disorders are possibly associated with LLD, some of these are increased hip pain and degeneration (especially involving the long leg). Increased risk of: knee injury, ITB syndrome, pronation and plantar fascitis, asymmetrical strength in lower extremity. Increased disc or vertebral degeneration. Symptoms vary between patients, some patients may complain of just headaches.
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.

how to grow taller at 17
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
Surgical options in leg length discrepancy treatment include procedures to lengthen the shorter leg, or shorten the longer leg. Your child's physician will choose the safest and most effective method based on the aforementioned factors. No matter the surgical procedure performed, physical therapy will be required after surgery in order to stretch muscles and help support the flexibility of the surrounding joints. Surgical shortening is safer than surgical lengthening and has fewer complications. Surgical procedures to shorten one leg include removing part of a bone, called a bone resection. They can also include epiphysiodesis or epiphyseal stapling, where the growth plate in a bone is tethered or stapled. This slows the rate of growth in the surgical leg.
Causes
Limb-length conditions can result from congenital disorders of the bones, muscles or joints, disuse or overuse of the bones, muscles or joints caused by illness or disease, diseases, such as bone cancer, Issues of the spine, shoulder or hip, traumatic injuries, such as severe fractures that damage growth plates.
Symptoms
The patient/athlete may present with an altered gait (such as limping) and/or scoliosis and/or low back pain. Lower extremity disorders are possibly associated with LLD, some of these are increased hip pain and degeneration (especially involving the long leg). Increased risk of: knee injury, ITB syndrome, pronation and plantar fascitis, asymmetrical strength in lower extremity. Increased disc or vertebral degeneration. Symptoms vary between patients, some patients may complain of just headaches.
Diagnosis
Infants, children or adolescents suspected of having a limb-length condition should receive an evaluation at the first sign of difficulty in using their arms or legs. In many cases, signs are subtle and only noticeable in certain situations, such as when buying clothing or playing sports. Proper initial assessments by qualified pediatric orthopedic providers can reduce the likelihood of long-term complications and increase the likelihood that less invasive management will be effective. In most cases, very mild limb length discrepancies require no formal treatment at all.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.
how to grow taller at 17
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
Ways To Fix Functional Leg Length Discrepancy
Overview
A Leg Length Inequality or Leg Length Discrepancy is exactly as it sounds. One or more bones (the Femur or thigh bone, the Tibia or shin bone, and/or the joint spacing within the knee) are unequal in total length when measured in comparison to the same structures on the opposite side. It is common for people to have one leg longer than the other. In fact, it is more typical to be asymmetrical than it is to be symmetrical.
Causes
LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio.
Symptoms
Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.

how do you get taller in a day?
Surgical Treatment
For discrepancies over five centimeters, more aggressive surgical procedures-specifically leg lengthening procedures-are typically required. The specifics of this operative procedure are beyond the scope of this informational page, but your child's physician will be able to discuss the details in reference to your child's specific problems when considered appropriate.
A Leg Length Inequality or Leg Length Discrepancy is exactly as it sounds. One or more bones (the Femur or thigh bone, the Tibia or shin bone, and/or the joint spacing within the knee) are unequal in total length when measured in comparison to the same structures on the opposite side. It is common for people to have one leg longer than the other. In fact, it is more typical to be asymmetrical than it is to be symmetrical.
Causes
LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio.
Symptoms
Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities.
Diagnosis
A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting.
Non Surgical Treatment
Treatment is based on an estimate of how great the difference in leg length will be when the child grows up, Small differences (a half inch or less) do not need treatment. Differences of a half to one inch may require a lift inside the shoe.
how do you get taller in a day?
Surgical Treatment
For discrepancies over five centimeters, more aggressive surgical procedures-specifically leg lengthening procedures-are typically required. The specifics of this operative procedure are beyond the scope of this informational page, but your child's physician will be able to discuss the details in reference to your child's specific problems when considered appropriate.
Dealing With Mortons Neuroma
Overview
 Morton's neuroma is named after Dr Morton who first described this condition in 1876. It is sometimes called Morton's metatarsalgia or interdigital neuroma. It is a condition that affects one of the common plantar digital nerves that run between the long bones (metatarsals) in the foot. It most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes. It can also affect the nerve between the second and third metatarsal bones, causing symptoms in the second and third toes. Morton's neuroma rarely affects the nerve between the first and second, or between the fourth and fifth, metatarsal bones. It tends to affect only one foot. It is rare to get two neuromas at the same time in the same foot.
Morton's neuroma is named after Dr Morton who first described this condition in 1876. It is sometimes called Morton's metatarsalgia or interdigital neuroma. It is a condition that affects one of the common plantar digital nerves that run between the long bones (metatarsals) in the foot. It most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes. It can also affect the nerve between the second and third metatarsal bones, causing symptoms in the second and third toes. Morton's neuroma rarely affects the nerve between the first and second, or between the fourth and fifth, metatarsal bones. It tends to affect only one foot. It is rare to get two neuromas at the same time in the same foot.
Causes
There are many reasons to develop a neuroma. Improper shoe gear is probably the most likely cause. Repetitive activity and excessive pressure on the ball of the foot are common. Heredity and genetic factors may also be involved. In many cases the structure of the foot may predispose the condition. Associated conditions that may cause neuroma include: bunion, hammer toes, ligament laxity, and/or a tight calf muscle. Some patients may have thinning of the fat pad on the ball of the foot, which may result in increased pressure of the nerves. Tight pointy shoes (and high heels) without padding may induce pain in the ball of the foot. Neuroma may occur suddenly, or develop over time.
Symptoms
A Morton's neuroma usually causes burning pain, numbness or tingling at the base of the third, fourth or second toes. Pain also can spread from the ball of the foot out to the tips of the toes. In some cases, there also is the sensation of a lump, a fold of sock or a "hot pebble" between the toes. Typically, the pain of a Morton's neuroma is relieved temporarily by taking off your shoes, flexing your toes and rubbing your feet. Symptoms may be aggravated by standing for prolonged periods or by wearing high heels or shoes with a narrow toe box.
Diagnosis
The doctor will perform an examination of your feet as well. He or she may palpate your feet and flex them in specific ways that will indicate the presence of a neuroma. X-rays are often used to rule out other problems, such as fractures, bone spurs, arthritis or other problems with the bones in the toes or foot. In some cases, an MRI (magnetic resonance imaging) may be helpful to confirm the presence of a neuroma.
Non Surgical Treatment
Orthotics and corticosteroid injections are widely used conservative treatments for Morton?s neuroma. In addition to traditional orthotic arch supports, a small foam or fabric pad may be positioned under the space between the two affected metatarsals, immediately behind the bone ends. This pad helps to splay the metatarsal bones and create more space for the nerve so as to relieve pressure and irritation. It may however also elicit mild uncomfortable sensations of its own, such as the feeling of having an awkward object under one's foot. Corticosteroid injections can relieve inflammation in some patients and help to end the symptoms. For some patients, however, the inflammation and pain recur after some weeks or months, and corticosteroids can only be used a limited number of times because they cause progressive degeneration of ligamentous and tendinous tissues.
Surgical Treatment
Surgery. This is the last and most permanent course of action. This surgery is used as a last resort as it often comes with a series of side affects including the risk of making the pain worse. This surgery can be performed by Orthopedic surgeons as well as Podiatric surgeons.
Morton's neuroma is named after Dr Morton who first described this condition in 1876. It is sometimes called Morton's metatarsalgia or interdigital neuroma. It is a condition that affects one of the common plantar digital nerves that run between the long bones (metatarsals) in the foot. It most commonly affects the nerve between the third and fourth metatarsal bones, causing pain and numbness in the third and fourth toes. It can also affect the nerve between the second and third metatarsal bones, causing symptoms in the second and third toes. Morton's neuroma rarely affects the nerve between the first and second, or between the fourth and fifth, metatarsal bones. It tends to affect only one foot. It is rare to get two neuromas at the same time in the same foot.Causes
There are many reasons to develop a neuroma. Improper shoe gear is probably the most likely cause. Repetitive activity and excessive pressure on the ball of the foot are common. Heredity and genetic factors may also be involved. In many cases the structure of the foot may predispose the condition. Associated conditions that may cause neuroma include: bunion, hammer toes, ligament laxity, and/or a tight calf muscle. Some patients may have thinning of the fat pad on the ball of the foot, which may result in increased pressure of the nerves. Tight pointy shoes (and high heels) without padding may induce pain in the ball of the foot. Neuroma may occur suddenly, or develop over time.
Symptoms
A Morton's neuroma usually causes burning pain, numbness or tingling at the base of the third, fourth or second toes. Pain also can spread from the ball of the foot out to the tips of the toes. In some cases, there also is the sensation of a lump, a fold of sock or a "hot pebble" between the toes. Typically, the pain of a Morton's neuroma is relieved temporarily by taking off your shoes, flexing your toes and rubbing your feet. Symptoms may be aggravated by standing for prolonged periods or by wearing high heels or shoes with a narrow toe box.
Diagnosis
The doctor will perform an examination of your feet as well. He or she may palpate your feet and flex them in specific ways that will indicate the presence of a neuroma. X-rays are often used to rule out other problems, such as fractures, bone spurs, arthritis or other problems with the bones in the toes or foot. In some cases, an MRI (magnetic resonance imaging) may be helpful to confirm the presence of a neuroma.
Non Surgical Treatment
Orthotics and corticosteroid injections are widely used conservative treatments for Morton?s neuroma. In addition to traditional orthotic arch supports, a small foam or fabric pad may be positioned under the space between the two affected metatarsals, immediately behind the bone ends. This pad helps to splay the metatarsal bones and create more space for the nerve so as to relieve pressure and irritation. It may however also elicit mild uncomfortable sensations of its own, such as the feeling of having an awkward object under one's foot. Corticosteroid injections can relieve inflammation in some patients and help to end the symptoms. For some patients, however, the inflammation and pain recur after some weeks or months, and corticosteroids can only be used a limited number of times because they cause progressive degeneration of ligamentous and tendinous tissues.
Surgical Treatment
Surgery. This is the last and most permanent course of action. This surgery is used as a last resort as it often comes with a series of side affects including the risk of making the pain worse. This surgery can be performed by Orthopedic surgeons as well as Podiatric surgeons.
How Shoe Lifts Remedy Leg Length Difference
There are actually two unique variations of leg length discrepancies, congenital and acquired. Congenital indicates you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental stages of aging, the human brain picks up on the step pattern and recognizes some variance. Our bodies typically adapts by tilting one shoulder to the "short" side. A difference of under a quarter inch is not blatantly irregular, demand Shoe Lifts to compensate and in most cases doesn't have a profound effect over a lifetime.

Leg length inequality goes typically undiscovered on a daily basis, yet this problem is easily fixed, and can eliminate numerous instances of back pain.
Treatment for leg length inequality typically consists of Shoe Lifts. These are generally cost-effective, in most cases priced at under twenty dollars, compared to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is easily the most common condition impacting people today. Around 80 million men and women are afflicted by back pain at some stage in their life. It is a problem which costs employers millions year after year as a result of lost time and production. New and improved treatment methods are always sought after in the hope of decreasing the economical influence this issue causes.

Men and women from all corners of the earth suffer the pain of foot ache due to leg length discrepancy. In a lot of these situations Shoe Lifts are usually of beneficial. The lifts are capable of decreasing any pain and discomfort in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic practitioners".
To be able to support the human body in a balanced fashion, the feet have a very important role to play. Inspite of that, it is often the most neglected area of the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This will cause other body parts like knees, ankles and backs to be impacted too. Shoe Lifts ensure that proper posture and balance are restored.
Leg length inequality goes typically undiscovered on a daily basis, yet this problem is easily fixed, and can eliminate numerous instances of back pain.
Treatment for leg length inequality typically consists of Shoe Lifts. These are generally cost-effective, in most cases priced at under twenty dollars, compared to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is easily the most common condition impacting people today. Around 80 million men and women are afflicted by back pain at some stage in their life. It is a problem which costs employers millions year after year as a result of lost time and production. New and improved treatment methods are always sought after in the hope of decreasing the economical influence this issue causes.
Men and women from all corners of the earth suffer the pain of foot ache due to leg length discrepancy. In a lot of these situations Shoe Lifts are usually of beneficial. The lifts are capable of decreasing any pain and discomfort in the feet. Shoe Lifts are recommended by numerous experienced orthopaedic practitioners".
To be able to support the human body in a balanced fashion, the feet have a very important role to play. Inspite of that, it is often the most neglected area of the body. Many people have flat-feet meaning there is unequal force exerted on the feet. This will cause other body parts like knees, ankles and backs to be impacted too. Shoe Lifts ensure that proper posture and balance are restored.
What Can Cause Inferior Calcaneal Spur
Overview
A heel spur occurs when calcium deposits build up on the underside of the heel bone, a process that usually occurs over a period of many months. Heel spurs are often caused by strains on foot muscles and ligaments, stretching of the plantar fascia, and repeated tearing of the membrane that covers the heel bone. Heel spurs are especially common among athletes whose activities include large amounts of running and jumping. Heel spurs often cause no symptoms but can be associated with intermittent pain, especially while walking, jogging, or running. Sharp pain in the heel can also be experienced when standing after sitting for a long period of time. Heel spurs can be a result of plantar fasciitis.
Causes
Heel spurs occur when calcium deposits build up on the underside of the heel bone, a process that usually occurs over a period of many months. Heel spurs are often caused by strains on foot muscles and ligaments, stretching of the plantar fascia, and repeated tearing of the membrane that covers the heel bone. Heel spurs are especially common among athletes whose activities include large amounts of running and jumping. Risk factors for heel spurs include walking gait abnormalities,which place excessive stress on the heel bone, ligaments, and nerves near the heel. Running or jogging, especially on hard surfaces. Poorly fitted or badly worn shoes, especially those lacking appropriate arch support. Excess weight and obesity. Other risk factors associated with plantar fasciitis include increasing age, which decreases plantar fascia flexibility and thins the heel's protective fat pad. Diabetes. Spending most of the day on one's feet. Frequent short bursts of physical activity. Having either flat feet or high arches.

Symptoms
The vast majority of people who have heel spurs feel the asscociated pain during their first steps in the morning. The pain is quite intense and felt either the bottom or front of the heel bone. Typically, the sharp pain diminishes after being up for a while but continues as a dull ache. The pain characteristically returns when first standing up after sitting for long periods.
Diagnosis
Sharp pain localized to the heel may be all a doctor needs to understand in order to diagnose the presence of heel spurs. However, you may also be sent to a radiologist for X-rays to confirm the presence of heel spurs.
Non Surgical Treatment
Elevation of the affected foot and leg at rest may diminish the pain. Applying gentle heat to the painful area may ease the pain by dilating local blood vessels. One also can protect the heel by placing a foam rubber pad in the heel of the shoe. A pad about one-half inch thick will raise the heel, shift the weight of the body forward, and protect the irritated muscles attached to the heel bone. The same effect can be achieved by using adhesive tape to turn the foot inward. Additional treatment may consist of a number of physical therapies, such as diathermy, ultrasound waves and whirlpool baths.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.